You might have heard a term “Psychedelic Renaissance.” In the West, research into the use of hallucinogens such as psilocybin, LSD and MDMA to treat mental illnesses such as PTSD, depression, and addictions is rapidly gaining momentum. A number of prestigious research and educational institutions, including Johns Hopkins University, New York University Langone Medical Center, and Mount Sinai School of Medicine in the USA, and the Imperial College London in the UK, are conducting research into hallucinogens. The treatment of PTSD with MDMA and depression with psilocybin are only a few of numerous ongoing clinical trials.
The laws surrounding hallucinogens have been rapidly changing over the past few years as well. In the US, State of Oregon, Denver, Oakland, Santa Cruz, Washington DC and Seattle have decriminalised the personal and non-commercial cultivation, possession, and use of hallucinogens. In the UK, Prime Minister Boris Johnson has shown interest in considering legalization of psilocybin.
There are high hopes for the medical usefulness of hallucinogens. However, it will be a few years at the earliest before these drugs are fully legalised and the regulatory framework is in place to allow legal access to these medicines for treatment. The only exception to this is ketamine.
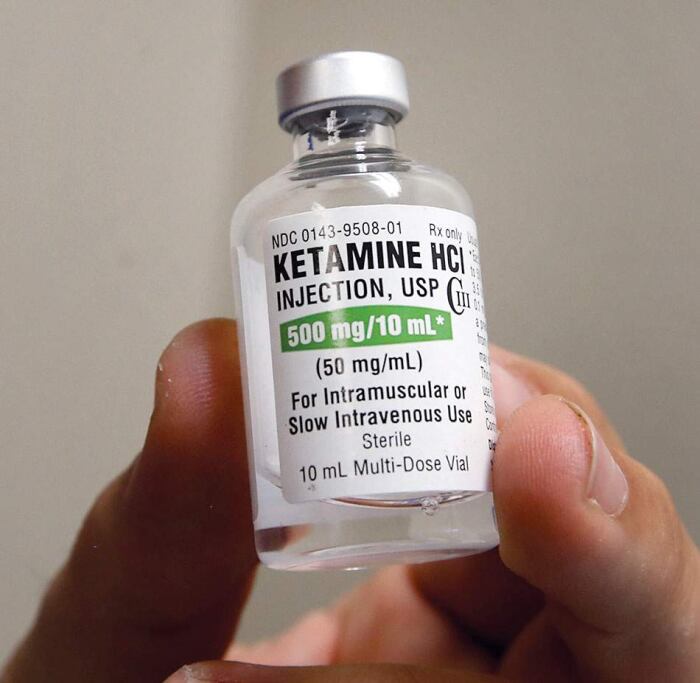
Ketamine is a dissociative drug originally approved in the US in 1970 as an anaesthetic, but in recent years its hallucinogen-like effects have been discovered to be useful in improving symptoms of depression. Although it is only officially approved as an anaesthetic, doctors are allowed to prescribe it off-label for depression and other psychiatric disorders. As a result, ketamine has become the focus of attention as a legally prescribable treatment, spearheading the movement to legalize hallucinogens, and many ketamine clinics have sprung up.
AIMS Institute in Seattle, with whom Green Zone Japan has a working relationship, is one of the integrative medicine clinics that offer treatment with ketamine, and we spoke to Dr. Sunil Aggarwal, co-founder of AIMS, to find out more.
GZJ: I would like to ask you about Ketamine Assisted Psychotherapy (KAP). How long have you been providing this treatment at AIMS Institute?
Sunil Aggarwal (SA): I personally have been using it for my patients since before I founded AIMS; I have been using ketamine as a treatment for PTSD, depression, and severe pain for about four years now. I think I had my first patient in 2017.
GZJ: We’ve heard that some people get this treatment as part of their cancer treatment. Does this mean that it is also effective in relieving the psychological pain associated with cancer?
SA: Yes, it can be useful in the treatment of cancer and a range of other serious chronic diseases that can leave patients feeling demoralised. For example, when a patient is diagnosed with a life-threatening illness such as cancer, they are very demoralised and their relationships, their outlook on life and the future, and many other things change.
Our approach comes from the tradition of treating the whole person, the patient, rather than the disease. The mind, the body, the whole person. Our hypothesis is that this kind of treatment not only reduces mental distress and reduces pessimism, but also enhances the immune system, so that there is a better response to the standard treatment of cancer – this is still a hypothesis, but we are trying to test it scientifically. But at least we know that treatment with hallucinogens, not just ketamine, can help improve mood disorders and demoralization in cancer patients.
GZJ: You mentioned earlier that you also use it for patients with PTSD and depression. Is that why some patients seek out ketamine therapy?
SA: Yes, it is. Ketamine-assisted psychotherapy is effective for all psychological problems that are not physical problems, such as PTSD, depression, anxiety, obsessive-compulsive disorder, even eating disorders and addictions — there is some early research on these. The scientific evidence is not 100% yet, and the FDA has not approved this indication, but it has been shown to help so many patients that the American Psychiatric Association has established guidelines so that doctors can use it correctly.
We have psychotherapists and psychiatric nurse practitioners at AIMS, and many of our staff are familiar with the treatment of trauma and know how to do mental health screening. We welcome the use of ketamine as a complementary therapy to regular treatment, and it is often sought by patients who have tried standard therapies such as cognitive behavioural therapy, mimetic therapy and medication. Unfortunately, these treatments are not very effective for PTSD, and neither for depression — depression is very difficult to treat. It is a complex problem, not just a biochemical problem, but one that is related also to the environment, the person’s circumstances, and traumatic experiences.
Ketamine as a psychotherapeutic treatment can help with these problems in a couple of levels. It changes the patterning of behaviour and thinking. So it’s a promising area, and I think in the future patients will be trying it first before the standard treatments.

GZJ: Let me ask about the actual process of receiving KAP. So there are two preparatory meetings before the ketamine is administered, correct?
SA: Yes, that’s right. The ketamine session takes a couple of hours and it’s a very intense experience, so we do a lot of preparation. It is important for the patient to have a good relationship with the person guiding the session, and the patient must feel comfortable that the guide understands them, as they are in a vulnerable position. It’s a very powerful healing process, but it has to be held well. That is why it is necessary for the patient and the guide to get to know each other first, rather than having a session at the first meeting.
The first step is screening to see whether ketamine is an appropriate treatment option for the patient. Are there any drug interactions with other medications the patient is taking? We also need to check the patient’s heart function, as their blood pressure may rise during the session. After these medical screenings, the patient will be screened to see if they are psychologically stable enough to undergo this treatment. This may be done in one session or in two. This is so that we know whether we can prescribe ketamine or not. Then we make sure they understand the risks and benefits and sign a consent form.
The next step is to prepare for the actual session. What specific issues do they want to address in this Ketamine session? ….. We will discuss whether it is a mood disorder, something they want to let go of, or a wound they want to heal. The doctor does not tell the patient to do this or that, but the patient and doctor participate in the treatment together. What do you (the patient) feel you need and how can I (the doctor) help you? This is called an ‘intention setting’ session. It’s about setting a goal. We also explain in detail how to prepare for the session. For example, you may not eat anything a few hours before the ketamine injection, you may want to drink lots of water but not too much so you don’t have to go to the bathroom during the session, or you may not want to take any other medicines that day or you may want to take them at different times, etc.
At this point, we know when the ketamine session will be. Before the actual administration, there is this preparation, then the administration, and then a later ‘integration’ session. This is a very transformative and intense experience, and we will supervise them before, during and after the treatment. Patients don’t just come to the clinic, get a dose of ketamine and call it a day.
GZJ: How many sessions does someone need if they have PTSD, addiction, or any other problem that they want to cure?
SA: This is still a new field, but generally speaking, ketamine has the ability to create a new mapping of brain function, or a new pattern in the neural network. And the changes are immediate. Animal studies have shown that new neural dendrites can be formed in less than 24 hours after ketamine administration. It releases what is called brain-derived neurotrophic factor.
If they just administer ketamine and don’t do any integration sessions or anything, this effect starts to weaken after about 10 days — 7 to 10 days. So we usually recommend that they do the first session, and then do an integration session within a few days or up to a week, and then follow with the second session. By that time the effects of the first session may have worn off, but the changes have started to happen. So we need to keep that momentum going. That’s where a second session comes in. We always recommend a minimum of two sessions.
You don’t need a preparation session for the second session. This means: preparation session → first dose → integration session → second dose → integration session. (Unless there is a huge time gap between the first and second doses.) Some people decide to have a session every other week, and have two, three, four or even five sessions. This all depends on the needs of the patient and how quickly they want the healing process to unfold. We may adjust the dosage along the way as well. Some people are very cautious and want to go slowly. So it’s different for everyone, but it usually takes two or three cycles to see improvement in a variety of conditions.
PTSD and addiction have what are called Cues (triggers) that need to be let go of, so there may be a need for structured support, such as an addiction counsellor or group therapy. There is a stage that patients go through, called behavioural activation, where you start to think that you want to behave in a certain way according to their values, and then they act on that. We need a place to support this change.
In addition to the sessions, I sometimes prescribe ketamine lozenges. By using it at home, you can prolong the changes brought about by the ketamine injection. Guided sessions are an expensive, time-consuming and intense experience, and they work very well in the early stages of treatment, but once the patient is used to them, they can use the lozenges too. The compound pharmacies will put flavouring on the ketamine powder and make it into a tablet that dissolves in the mouth. You swish it around in your mouth for about 10 minutes to maximise absorption.
GZJ: Does the patient decide when they use it at home?
SA: We do give guidance. For example, if they have regular sessions in the clinic, they might want to do it once a week at home. We give them guidance on how to do it safely, what music to play, what eyeshades to wear, things like that. Some people need someone to be with them. And then we do a follow-up integration session. They need a place to process the material that has come to the surface through the use of ketamine.
Patients use the lozenges at home once, twice or even three times a week, depending on their needs. It is very effective when combined with injection sessions. It is also possible to combine it with other treatments.
We also offer a program of ketamine injection sessions in small groups. We inject a number of people who have already had experience with ketamine at the same time. We set an intention as a group, we do a session, and then a week later we do another integration session as a group. This is a way of taking advantage of the strengths of group therapy, which can be very effective for some conditions. It’s also less expensive, because it’s more efficient than one-to-one sessions. We are not alone, many ketamine clinics in the USA and around the world use this method.
Many clinics still use intravenous ketamine, but we don’t use IVs for high-dose sessions, because it feels too medicalized to be hooked up to an IV bag and because we want to go deeper, into the patient’s life and beliefs. Many IV clinics don’t even have a guide or preparation with the patient. That’s the difference between our approach and theirs. But there are clinics all over the world that give ketamine infusions, aren’t there some in Japan?
GZJ: No, I don’t think so.
SA: Is that so? Ketamine is not listed as a controlled substance by the WHO, and it is one of the most accessible drugs in the world.
Author's note: In Japan, a new drug is being developed based on the R form of ketamine, as opposed to the S form used in the West. https://www.otsuka.co.jp/company/newsreleases/2021/20210316_1.html
GZJ: Would you tell us about the dosage?
SA: Ketamine in high doses is used as an anaesthetic. Ketamine is the most widely used anaesthetic in the world. It’s easy to use because it doesn’t inhibit breathing and doesn’t need any extra equipment. This is why it is used in developing countries where there are no ventilators.
It is used in lower doses for psychotherapy. Basically, the total dose is determined by how many milligrams are taken per kilogram of body weight. A very low dose for analgesia is about 0.1 to 0.3 milligrams per kilogram of body weight; 0.5 milligrams is the most commonly used dose for intravenous infusion, which is not very psychoactive and is used for repeated infusions; there is a gradation of 0.8 to 1.0 milligrams, and then 1.0 to 1.5 milligrams, which is our general dosage. But some patients go up to 2.0 or even 2.1 milligrams, and above 2.5 or 3.0 milligrams they fall asleep and remember very little.
We don’t want to make the patient lose consciousness, rather we want to make a change there. This is the twilight zone, the altered state of consciousness, between the waking and dreaming states. This is where a very powerful healing happens and has been used in traditional medicine since ancient times. For example, psilocybin has been used for this purpose for a long time, but in 1970 it was made illegal to use it as a medicine, so it cannot be used for any other purpose than research. We’re trying to change that, though.
GZJ: Yes, I’d love to hear about that.
<To be continued in Part 2>
In the second part of this article, we will talk about the ongoing lawsuit filed by Dr. Aggarwal against the DEA for the use of psilocybin.
 Interviewer:Naoko Miki. Book translator, co-founder of Green Zone Japan. Among the books she translated are; “Marijuana is Safer: So Why Are We Driving People to Drink? ,” “Cannabis for the Treatment of Cancer: The Anticancer Activity of Phytocannabinoids and Endocannabinoids” and “Healing with CBD: How Cannabidiol Can Transform Your Health without the High.”
Interviewer:Naoko Miki. Book translator, co-founder of Green Zone Japan. Among the books she translated are; “Marijuana is Safer: So Why Are We Driving People to Drink? ,” “Cannabis for the Treatment of Cancer: The Anticancer Activity of Phytocannabinoids and Endocannabinoids” and “Healing with CBD: How Cannabidiol Can Transform Your Health without the High.”


コメントを残す